
Introduction
Digestive health issues are extremely common and can significantly impact a person’s quality of life. Two terms that frequently arise in discussions about gastrointestinal problems are Irritable Bowel Syndrome (IBS) and Inflammatory Bowel Disease (IBD).
While they may share certain symptoms, their underlying causes, diagnostic approaches, and management strategies differ substantially.
As a doctor, I often encounter questions about how to differentiate between the two and how to manage their symptoms effectively.
In this article, we’ll explore IBS vs IBD in detail—covering their definitions, causes, symptoms, diagnosis, and management strategies.
Irritable Bowel Syndrome (IBS) and Inflammatory Bowel Disease (IBD)
Understanding IBS (Irritable Bowel Syndrome)
1. What Is IBS?
Irritable Bowel Syndrome (IBS) is a functional gastrointestinal disorder, meaning the structure of the bowel appears normal, but it does not function as it should. It affects the large intestine (colon) and is characterized by chronic abdominal pain, bloating, and altered bowel habits.
2. Causes and Risk Factors
- Motility issues: Abnormal intestinal muscle contractions can speed up or slow down movement through the gut.
- Gut-brain axis dysregulation: Stress and emotional factors can alter the way the brain communicates with the digestive tract.
- Food sensitivities: Certain foods (like dairy or high FODMAP foods) can exacerbate IBS symptoms.
- Gut microbiome imbalance: Disruptions in the gut flora can play a role.
- Genetic predisposition: A family history may increase the risk.
3. Common Symptoms
- Abdominal pain or cramping (often relieved by bowel movements)
- Bloating and excess gas
- Diarrhea (IBS-D), constipation (IBS-C), or alternating diarrhea and constipation (IBS-M)
- Mucus in the stool
- A feeling of incomplete evacuation after a bowel movement
4. Diagnosis of IBS
- Rome IV Criteria: IBS is typically diagnosed based on symptom patterns rather than specific biochemical markers. According to the Rome IV criteria, a patient must have recurrent abdominal pain at least 1 day per week in the last 3 months, associated with two or more of the following:
- Related to defecation
- Change in frequency of stool
- Change in form (appearance) of stool
- Exclusion of Other Conditions: Tests such as blood work, stool studies, and sometimes colonoscopy may be conducted to rule out other conditions like celiac disease or IBD.
Understanding IBD (Inflammatory Bowel Disease)
1. What Is IBD?
Inflammatory Bowel Disease (IBD) is an umbrella term for conditions characterized by chronic inflammation of the gastrointestinal tract, most commonly:
- Crohn’s Disease: Can affect any part of the GI tract from mouth to anus, often involving deeper layers of the intestinal lining.
- Ulcerative Colitis (UC): Involves chronic inflammation and ulcers primarily in the colon and rectum, usually affecting the mucosal layer.
2. Causes and Risk Factors
- Autoimmune Component: The immune system mistakenly attacks the gut lining, causing inflammation.
- Genetic Predisposition: IBD often runs in families.
- Environmental Triggers: Diet, lifestyle factors, and certain medications can influence disease onset and flare-ups.
- Gut Microbiome: An imbalance in the intestinal microbiota can contribute to inflammation.
3. Common Symptoms
- Persistent diarrhea (which can be bloody, especially in UC)
- Abdominal pain and cramping
- Urgency and frequent bowel movements
- Weight loss and malnutrition
- Fatigue and sometimes fever
4. Diagnosis of IBD
- Endoscopic Evaluation: Colonoscopy with biopsy is crucial to visualize inflammation and obtain tissue samples.
- Imaging Studies: CT or MRI can show the extent and severity of inflammation.
- Laboratory Tests: Inflammatory markers like C-reactive protein (CRP) and Erythrocyte Sedimentation Rate (ESR) are often elevated. Stool calprotectin is another useful marker.
- Histopathology: Biopsies help differentiate between Crohn’s Disease and Ulcerative Colitis.
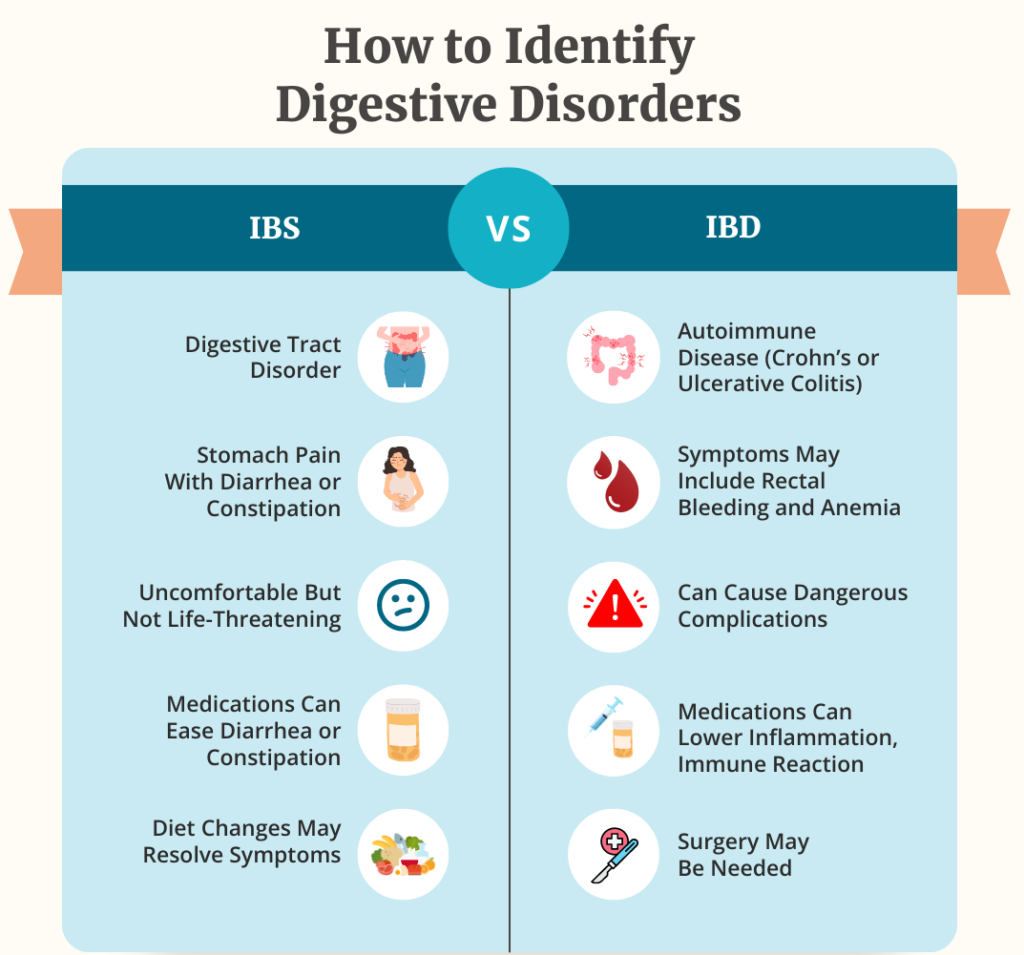
Key Differences Between IBS and IBD
| Aspect | IBS | IBD |
|---|---|---|
| Nature of the disorder | Functional disorder (no visible inflammation) | Chronic inflammatory disorder |
| Affected regions | Primarily the large intestine | Crohn’s can affect entire GI tract; UC affects colon/rectum |
| Structural changes | Usually normal bowel tissue on exam | Visible damage, inflammation, ulcers |
| Symptoms | Abdominal pain, bloating, diarrhea/constipation | Diarrhea (often bloody), abdominal pain, weight loss |
| Diagnoses tests | Based on symptom criteria (Rome IV), exclusion | Colonoscopy, imaging, lab markers (CRP, ESR), biopsies |
| Long-term complications | Rare to cause structural damage | Can lead to strictures, fistulas, malnutrition, cancer risk |
Management Strategies
1. Managing IBS
- Dietary Modifications
- Low FODMAP Diet: Reducing certain fermentable carbohydrates (e.g., fructose, lactose, fructans, galactans) can alleviate symptoms.
- Fiber Intake: Increasing soluble fiber (found in oats, peas, beans, apples) can improve bowel regularity. Some individuals with IBS-C benefit from fiber, but for IBS-D, too much fiber might worsen symptoms.
- Identifying Trigger Foods: Common triggers include caffeine, dairy, and spicy or fatty foods. An elimination diet can help identify specific triggers.
- Stress Management
- Cognitive Behavioral Therapy (CBT): Helps in developing coping mechanisms for chronic pain and stress.
- Mindfulness and Relaxation Techniques: Yoga, meditation, and deep breathing exercises can ease the gut-brain axis dysregulation.
- Medications
- Antispasmodics: Such as hyoscine (Buscopan) or peppermint oil to reduce cramping.
- Laxatives or Antidiarrheal Agents: Depending on whether constipation or diarrhea predominates.
- Low-dose Antidepressants: Tricyclic antidepressants or SSRIs can help alleviate pain and regulate bowel habits in some cases.
- Probiotics
- Certain probiotic strains may help restore gut flora balance, though evidence varies.
2. Managing IBD
- Medications
- Aminosalicylates (5-ASA): Often first-line for mild to moderate Ulcerative Colitis.
- Corticosteroids: For acute flare-ups to reduce inflammation quickly.
- Immunomodulators: Azathioprine, 6-mercaptopurine, or methotrexate for maintaining remission and reducing steroid dependence.
- Biologic Therapies: Anti-TNF agents (e.g., infliximab), anti-integrins (vedolizumab), and other targeted therapies for moderate to severe cases.
- Dietary Considerations
- Nutrient-Rich Foods: Ensuring adequate protein, vitamins, and minerals. Malabsorption can occur in IBD, especially Crohn’s.
- Identifying Triggers: Some people may benefit from limiting high-residue foods during flare-ups.
- Enteral Nutrition: In certain cases, specialized liquid nutrition or feeding tubes are used for bowel rest and nourishment.
- Lifestyle & Support
- Quit Smoking: Particularly beneficial in Crohn’s Disease, as smoking can worsen the course of the disease.
- Regular Exercise: Low-impact activities like walking or swimming can help maintain overall health.
- Psychological Support: Chronic illness can affect mental health; counseling or support groups are helpful.
- Surgical Options
- Ulcerative Colitis: Colectomy (removal of the colon) can be curative.
- Crohn’s Disease: Surgery may remove strictured or diseased sections, but recurrence can happen elsewhere in the GI tract.
Additional Tips for Symptom Relief
- Keep a Symptom Diary: Track foods, stress levels, and bowel habits to identify patterns.
- Stay Hydrated: Particularly important for those with diarrhea to prevent dehydration.
- Sleep and Stress: Adequate rest and stress reduction techniques go a long way in managing flare-ups and overall well-being.
- Regular Follow-ups: Conditions like IBD require ongoing monitoring. Even IBS can change over time, and personalized treatment plans might need adjustment.
Conclusion
Although IBS and IBD share some overlapping symptoms—like abdominal pain, diarrhea, and bloating—their underlying mechanisms and long-term implications are distinct. IBS is a functional disorder primarily managed through dietary and lifestyle changes, as well as stress reduction and symptom-targeted medications. IBD, on the other hand, involves an inflammatory process that may require medications to control the immune response, address acute flare-ups, and, in some cases, surgery.
If you or someone you know struggles with persistent gastrointestinal symptoms, it’s crucial to seek professional evaluation. An accurate diagnosis is the first step in finding the right treatment and achieving relief. With proper management, most individuals with IBS or IBD can lead healthy and fulfilling lives.
For more information or personalized guidance, feel free to contact us at Vardham Health. As a doctor, I encourage you to stay informed, stay proactive, and partner with healthcare professionals to optimize your digestive health.
Understanding Pain in the Lower Abdomen for Females: Causes, Symptoms, and Solutions
Maintaining Gastrointestinal Health Through Diet
Foods to Avoid and Include for Incompetent Cervix: A Detailed Guide